

Abstract
Objective. Powered exoskeletons promise to increase the quality of life of people with lower-body paralysis or weakened legs by assisting or restoring legged mobility while providing health benefits across multiple physiological systems. Here, a systematic review of the literature on powered exoskeletons addressed critical questions: What is the current evidence of clinical efficacy for lower-limb powered exoskeletons? What are the benefits and risks for individuals with spinal cord injury (SCI)? What are the levels of injury considered in such studies? What are their outcome measures? What are the opportunities for the next generation exoskeletons? Approach. A systematic search of online databases was performed to identify clinical trials and safety or efficacy studies with lower-limb powered exoskeletons for individuals with SCI. Twenty-two studies with eight powered exoskeletons thus selected, were analyzed based on the protocol design, subject demographics, study duration, and primary/secondary outcome measures for assessing exoskeleton's performance in SCI subjects. Main results. Findings show that the level of injury varies across studies, with T10 injuries being represented in 45.4% of the studies. A categorical breakdown of outcome measures revealed 63% of these measures were gait and ambulation related, followed by energy expenditure (16%), physiological improvements (13%), and usability and comfort (8%). Moreover, outcome measures varied across studies, and none had measures spanning every category, making comparisons difficult. Significance. This review of the literature shows that a majority of current studies focus on thoracic level injury as well as there is an emphasis on ambulatory-related primary outcome measures. Future research should: 1) develop criteria for optimal selection and training of patients most likely to benefit from this technology, 2) design multimodal gait intention detection systems that engage and empower the user, 3) develop real-time monitoring and diagnostic capabilities, and 4) adopt comprehensive metrics for assessing safety, benefits, and usability.
Export citation and abstract BibTeX RIS
1. Introduction
In 2014, spinal cord injuries (SCI) were reported to affect approximately 276 000 persons in the United States, with approximately 12 500 new SCI cases each year (NSCISC 2015). According to the University of Alabama National Spinal Cord Injury Statistical Center and the Centers for Disease Control and Prevention (CDC), the costs of living with SCI can be considerable, and vary greatly due to the severity, age of injury and loss of income. The lifetime costs for an individual that can be directly linked to high tetraplegia can reach $4.7 million (NSCISC 2015). SCI has a significant impact on a person's quality of life (QOL) and health status (Behrman and Harkema 2000). Decreased mobility is likely related to higher blood pressure, shorter life expectancy, social stigma and increased rates of depression (Parent et al 2011). Thus, walking is usually cited as one of the primary goals of rehabilitation due to the physiological and social implications (Ditunno et al 2008, Calhoun et al 2013).
Gait therapy is a rehabilitation method used to improve general health and walking ability of individuals with lower limb dysfunction. Even in the case of complete SCI subjects with no voluntary control below the level of the lesion, manually-assisted or robot assisted locomotor training can result in beneficial effects in cardiovascular and musculoskeletal systems (Hesse 2001, Hubli and Dietz 2013). Robotic gait assistance allows increased training duration, reproducible gait patterns as well as close monitoring of patient progress during therapy (Hidler and Sainburg 2011). Both the manual method, in which physical therapists articulate the individual's lower limbs by hand to maintain a correct walking gait (Hesse 2001), and robotic gait method have shown improved patient outcomes but there has not been enough statistical evidence to definitively demonstrate the advantages of robotic training (Yang and Musselman 2012). More recently, research has focused on engaging the individual and adjusting limb actuation based on the need and input from the user. Thus, impedance-controlled robotic gait allows for an assist-as-needed approach and is meant to keep the user actively engaged in the walking process with the expectation that rehabilitation will have a greater impact if the individual is more focused on the task. The effectiveness of impedance control has been demonstrated, but no comparison has yet been done to show any statistically significant advantage over other methods (Fleerkotte et al 2014).
With recent developments in robotic technologies, powered exoskeletons have emerged as practical devices for assisting individuals with lower limb paralysis or weakened limbs and as devices to assist and support the work of physical therapists. The US Food and Drug Administration (FDA) have recently approved a de novo product classification for powered exoskeletons (product code PHL, a Class II device with special controls) (Food and Drug Administration, HHS 2015). Unfortunately, while exoskeleton technology continues to advance and psychological as well as physiological benefits of legged mobility are likely, the anticipated benefits across multiple physiological systems remain largely unproven. Moreover, studies are required to evaluate the potential risks of deploying this technology outside the clinic, including falls, changes in blood pressure (diastolic hypertension and hypotension) and heart rate, skin abrasions, bruising, pressure sores, increased spasticity, lightheadedness, and soft tissue injury.
This systematic review of powered exoskeletons for bipedal locomotion in SCI patients was undertaken to address five specific questions: (1) What is current evidence of clinical efficacy for lower-limb powered exoskeleton? (2) What are the benefits and risks for individuals with spinal cord injury? (3) What are the levels of injury considered in such studies? (4) What are their outcome measures? (5) What are the opportunities for the next generation exoskeletons?
2. What constitutes a powered exoskeleton?
According to the FDA's definition, a powered exoskeleton is 'a prescription device that is composed of an external, powered, motorized orthosis used for medical purposes that is placed over a person's paralyzed or weakened limbs for the purpose of providing ambulation' (Food and Drug Administration, HHS 2015). This definition differs from the terminology proposed by (Herr 2009), which restricts the term exoskeleton to a device that enhances the physical capabilities of an able-bodied user, but is consistent with the view of an orthosis as a device used to assist a person with an impairment of the limbs.
For the purpose of this review, the NIH revised definition of a clinical trial was used as inclusion criteria for the selection of clinical studies of powered exoskeletons. The NIH defines a clinical trial as 'a research study in which one or more human subjects are prospectively assigned to one or more interventions (which may include placebo or other control) to evaluate the effects of those interventions on health-related biomedical or behavioral outcomes' (http://grants.nih.gov/grants/guide/notice-files/NOT-OD-15-015.html). Thus, a clinical study included in this review is a research study in which one or more human subjects are prospectively and necessarily assigned to a powered exoskeleton for over-ground legged mobility to evaluate the effects of the intervention(s) on functional, physiological, behavioral, or psychological outcomes. Additionally, to create a more comprehensive review of current literature, a powered exoskeleton study was selected for inclusion in this review if the purpose of the study was to determine whether the powered exoskeleton intervention was safe, efficacious, and/or effective, and the target population was SCI. Moreover, only peer-reviewed journal and conference papers were included in this review. However, studies that only applied the exoskeleton for purposes of evaluating the feasibility or performance of the device, absent of any monitoring of the individual for physiological changes, were excluded from review. Likewise, review papers or book chapters or non-English articles were also excluded.
We also excluded passive orthoses such as ankle-foot orthoses (AFOs) and reciprocating gait orthoses unless they were part of a powered exoskeleton. For this information, the reader is directed to several published reviews surveying the state-of-the-art for lower-extremity powered exoskeletons (Ferris et al 2007, Dollar and Herr 2008, Pons 2008, Yang et al 2008, Bogue 2009, Herr 2009). While there are several studies reviewing the overall design and control strategy of different types of exoskeletons from an engineering perspective (Jimenez-Fabian and Verlinden 2012, Tucker et al 2015), including gait speed (Louie et al 2015), few have analyzed the rehabilitation efficacy with these devices (Mehrholz and Pohl 2012, Federici et al 2015, Lajeunesse et al 2015). However, to our knowledge, no study has examined in detail the primary and secondary outcomes of the published studies and clinical trials with powered exoskeletons for the SCI community.
2.1. Search strategy
We searched four online databases until 8th December, 2015 and retrieved 430 publications: 43 belonging to PubMed, 134 in Web of Science, 80 in ProQuest, and 123 in Scopus. The following search terms were used in all fields: (robotic OR power* OR over-ground OR walk* OR gait) AND (exoskeleton OR exoskeletal OR orthos*) AND (spinal cord injury OR SCI OR paraplegia OR tetraplegia) AND (leg OR lower AND (limb OR extremity)) AND (rehabilitation* OR clinical*).
After removing duplicate references, 327 references were retained. These references were divided into three groups and each group was independently reviewed by two authors. Each author screened the title and abstracts of the assigned studies and determined their eligibility for the review. Disagreements between authors were resolved by mutual discussion. Studies selected by each group were then pooled together to yield 11 studies. A separate literature search on Google Scholar was conducted to find recent articles published since 2012, which may have been missed by other databases. This search resulted in 2100 results (excluding patents), which were further filtered by adding the exoskeleton device names, previously identified to the search terms that had been used in the initial search using the PubMed, Web of Science, ProQuest and Scopus databases. Since Google Scholar restricts search terms to 256 characters (Boeker et al 2013), we added the exoskeleton names to the search terms one at a time, i.e. (ORIGINAL_SEARCH_TERMS) AND (EXOSKELETON_NAME). Hand searches of reference lists from retrieved articles were completed. After screening for eligibility, 11 additional articles were selected and combined with the previously selected studies. Thus, in the end 22 studies were selected that met our inclusion criteria and were included in this review. We also searched ClinicalTrials.gov for registered studies with exoskeletons identified from the selected studies (see table 1).
Table 1. Summary of powered exoskeletons for individuals with SCI.
| Exoskeleton |

|
|

|

|
|

|

|

|
|---|---|---|---|---|---|---|---|---|
| Degrees of freedom | K | HKA | HKA | HK | KA | HKA | HaHKA | HKA |
| Weight-bearing devices | W | C | W/C/S | W/C | W/C | C | S | W/B |
| Sensor measurements | JA, JT, FF | AJA, ACF, FF, Acc/Ori (arm) | EMG, JA, FF, Acc | JA, Acc, Ori | JA, FF, IT, Ori | JA, FF, Ori | IT, JA | JA, JT |
| Device weight (kg) | 3.6 | 20 | 15 | 12 | 9.2 | 23 | ? | 13 |
| User height (cm) limit | 153–182 | 158–188 | 145–185 | 155–191 | <1.85 | 160–190 | ? | 145–180 |
| User weight (kg) limit | 136 | 100 | 80 | 113 | 90 | 100 | ? | 80 |
| Gait initiation mode | Foot sensors and knee extension | 1. Body tilt | Knee EMG activation | Body tilt | Button push | Body tilt | ? | Button push |
| 2. Button push | ||||||||
| Unique features | Unilateral | — | — | — | Hybrid (FES) | — | Hybrid (FES), active bodyweight support suspension harness moves with exoskeleton | Frame fits between legs, easy to don within wheerchair |
| ClinicalTrials.gov registration ID | NCT01701388 | — | NCT02202538 | — | NCT02322125 | — | ||
| NCT02324322 | NCT01943669 | |||||||
| NCT02132702 | NCT02118194 | |||||||
| NCT02065830 | NCT02104622 | |||||||
| NCT01251549 | ||||||||
| NCT00627107 | ||||||||
| NCT01454570 |
Note: Degrees of freedom: (Bilateral) Ha-hip ab/adduction, Hr-hip medial/lateral rotation, H-hip (sagittal), K-knee (sagittal), A-ankle (sagittal), Av-ankle in/eversion, underline-passive.Weight-bearing devices: C-crutches, W-walker, B-parallel safety bars, S-suspension harness.Sensor measurements: EMG-electromyography, JA-joint angle, AJA-arm joint angle, ACF-arm crutches force, IT-interaction torque, JT-joint torque, FF-foot contacting force/pressure, Acc-acceleration, Ori-orientation.
3. Wearable robots or powered exoskeleton technologies
While there are numerous wearable robots or powered exoskeletons for legged mobility under development, under clinical trials with human subjects, or already marketed; we identified studies with eight3 exoskeleton devices that fit the inclusion criteria. These exoskeletons are described below.
3.1. Bionic Leg (AlterG Inc. Fremont, CA, USA, http://alterg.com/products/bionic-leg/professional-physical-therapy/)
The AlterG Bionic Leg (formerly Tibion Bionic Leg) is a unilateral robotic knee orthoses (RKO) for individuals with asymmetric lower-limb motor impairments, for example the Brown-Sequared syndrome (Bishop et al 2012). The device is designed to assist the user during sit-to-stand transitions, over-ground walking and stair climbing/descent. It uses four force sensors mounted on a foot plate which detect the amount and time of weight-bearing through the foot. Additional sensors which measure the knee angle and the extension force provided by the actuators are also incorporated. The user interface allows a trained therapist to adjust the amount of assistance and/or resistance provided by the device, device range-of-motion as well as minimum force required to activate the device. When the device is inactive, it is back-drivable which functions as a safety feature and allows therapist to position the lower extremity in weight-bearing exercise mode. The device is untethered from any cords and contains its own battery power that can lasts up to 2–3 h. For ensuring patient stability and safety, it is operated with a walker (Bishop et al 2012).
3.2. Ekso exoskeleton (Eksobionics Ltd, Richmond, CA, USA; http://eksobionics.com/)
Ekso is a wearable lower extremity robotic exoskeleton with two legs connected to a torso structure containing the computer and batteries. The torso is aligned to the user's lower back, and the exoskeleton legs are fastened to the user's legs by hook-and-loop fastener straps that align the user's lower back and joints with those of the device. Two additional straps are tightened over the user's shoulders to help support the torso structure. The device has powered (bilaterally) hip and knee joints in the sagittal plane and other movement directions are restricted. The ankle joints of the exoskeleton allow passive (spring) movement limited to the sagittal plane. Currently, Ekso has four walk modes: in the first two walk modes, either a physical therapist or the user actuates sit-to-stand and steps with a button push; whereas in the other two walk modes, gait intent detection to command the exoskeleton is accomplished by detecting the forward and lateral movement of the user's hips (to accomplish weight shift); or by the user's weight shift and the initiation of forward leg movement. Ekso requires walking aids using provided crutches to ensure stability and safety of the user; the bottoms of the crutches are fitted with force sensors to ensure firm placement on the ground and at least partial weight-bearing. A step will not be triggered unless both crutches are firmly on the ground. Additionally, the controller uses a hierarchical finite state machine to transition between the different movements without forcing the user into unsafe positions (Strausser and Kazerooni 2011). According to the manufacturer, newer versions of Ekso are capable of providing variable assist or assist-as-needed power to the user. Thus, therapists have the option to assign a specific amount of power contribution to augment their patients' efforts, or to allow the exoskeleton to dynamically adjust to their needs in real-time. Ekso has not currently been approved by the FDA as a Class II device as a powered exoskeleton, but the company has submitted a 510(k) application and has been allowed to continue device marketing during the review process.
3.3. Hybrid assisted limb (HAL; Cyberdyne Inc., Tsukuba, Japan; http://cyberdyne.jp/english/)
HAL is a bilateral lower-limb exoskeleton with three active degrees of freedom for actuating the hip, knee and ankle joints. The HAL system comes in different models, allowing single joint or full body support during walking, standing and sitting (Suzuki et al 2007). It consists of six main parts: controller, battery, power unit, electromyography (EMG) sensors, angular/acceleration sensors, and floor reaction force sensors (Sankai 2011). The control system receives data from EMG, angle/acceleration, and force sensors and computes the necessary forces to complement the user's actions. The use of EMG to determine user's intention, instead of a joystick or other manual controller is beneficial, since it allows the user to operate the device by simply attempting to initiate a movement. Currently, the battery life allows 2 h 40 min operation time. For patient safety and stability during walking, HAL is used with a walker or cane (Kubota et al 2013). The HAL exoskeleton is commercially marketed in Japan and Europe as a medical prescription device developed for people who have lower-limb disorders and people whose legs are weakening. The device has been certified (ISO13485) under the European Medical Device Directive (CE 0197). The manufacturer has applied for marketing authorization of HAL for medical use as a new medical device for orphan neural-muscular diseases, such as muscular dystrophy, amyotrophic lateral sclerosis (ALS) under Japan's Pharmaceutical and Medical Device Law.
3.4. Indego (Parker Hannifin Corp., Macedonia, OH, USA; http://indego.com/indego/en/home)
The Indego modular exoskeleton is comprised of powered bilateral hip and knee joints, and it incorporates built-in AFOs that provide ankle stability and exoskeleton weight transfer to the ground (Hartigan et al 2015). The exoskeleton's hip, upper and lower leg modules assemble via quick-connects to enable easy donning, doffing, and transportation as well as compact storage of the device. Its slim profile is compatible with standard mobility aids and can be worn while seated in a wheelchair. The exoskeleton enables sitting, walking, standing, sit-to-stand, stand-to-walk, walk-to-stand, and stand-to-sit transitions. Intent detection for locomotive and non-locomotive tasks is based on the user's ability to affect his center of pressure (CoP) via the use of the upper body in combination with a stability aid such as a walker. The controller uses the distance between the CoP and the location of the forward ankle joint as the primary command input to the device. This requires the user to tilt the body forward or backward such that the CoP moves in an anterior or posterior direction, which commands the controller to transition to a different movement mode. As a safety measure there are brakes at the knee joints to prevent knee buckling in case of power failure (Quintero et al 2011). On 8 March 2016, the FDA released its summary of the 510(k) premarket notification for the Indego exoskeleton (http://www.accessdata.fda.gov/cdrh_docs/pdf15/k152416.pdf). The FDA reviewed the Section 510(k) premarket notification of intent to market the Indego device and has determined the Indego, as designed and manufactured, meets the Special Controls specified in 21 CFR 890.3480, and is determined to be substantially equivalent to the referenced predicate device (ReWalk exoskeleton from Argo Medical Technologies), thus allowing Parker Hannifin Corporation to market the Indego device, subject to the general controls provisions of the Federal Food, Drug, and Cosmetic Act.
3.5. Kinesis (Technaid, Madrid, Spain; http://technaid.com/en/products/exoskeleton)
Kinesis is a lower limb rehabilitation robot designed for providing hybrid therapy of walking to patients with incomplete spinal cord injury. The target population is patients with a prognosis for functional recovery of walking, i.e. patients who can walk short distances but depend on the wheelchair for community ambulation, usually with some preservation of hip flexor function. Kinesis is a knee-ankle-foot exoskeleton, equipped with an active actuator in the knee, a passive elastic actuator at the ankle for plantar and dorsal flexion, and is equipped with force-sensitive resistors to detect foot-ground contact, potentiometers to monitor joint angular position, and embedded strain gauge-based Wheatstone bridge to measure user-robot interaction torques (del-Ama et al 2012). A biologically inspired mechanism for the knee joint allows the joint axis to follow the translational motion of the physiological knee joint axis, improving kinematic compatibility between the orthosis and the subject with respect to a single-axis joint. As a hybrid-therapy system, Kinesis can provide functional electrical stimulation (FES) to the knee extensor (rectus femoris and vastus lateralis) and flexor (semitendinosus and biceps femoris) muscles through surface electrodes. The main controller for Kinesis consists of four components: a robotic or joint controller, an FES controller, a muscle fatigue estimator, and a finite state machine to coordinate the FES and joint controllers. Kinesis uses shared control to operate the robot actuators and FES of knee joint muscles while managing muscle fatigue. The FES controller is only active during swing phases of gait, while a PID controller for knee extensor muscles is active across the full gait cycle. The Kinesis hybrid controller works to minimize the interaction forces between the user's body and the exoskeleton (del-Ama et al 2014, 2015). The Kinesis has several built-in safety measures including: mechanical stops in the physiological limits of motion at the robotic joints; software limits for maximum and minimum positions in the admittance controller for the knee joint, maximum output torques, and FES pulse width and amplitude modulation; and a mechanical safety button to physically disconnect power from the entire hardware (del-Ama et al 2014).
3.6. ReWalk (Argo Medical Technologies Ltd, Yokneam Ilit, Israel; http://rewalk.com/)
The ReWalk is an end-effector-based robot with footplates placed on a double crank and rocker gear system. The device is comprised of a powered exoskeleton that bilaterally controls the movements at the hip and knee joints (ankles are articulated with spring-assisted dorsiflexion), a battery unit, and a computer-based controller contained in a backpack, a wireless mode selector, and sensors that measure upper-body tilt angle, joint angles, and ground contact. The exoskeleton is articulated to footplates distally and to a sacral band proximally. The device senses the patient's movements to control externally powered gait using closed-loop control algorithms (Zeilig et al 2012). Thus, for example in the 'walk' mode, forward flexion of the upper body is detected by the tilt sensor, which triggers a step. The gait is a three-point pattern, advancing one step at a time. Additional modes include sit-to-stand, stand-to-sit, up steps, and down steps. The maximal walking velocity in the latest model (ReWalk 6.0) is 2.6 km h−1 (Yang et al 2015). Undesirable rapid hip and knee flexion, as may occur in a fall, is prevented by software, which also provides a controlled speed during stand-to-sit movements. The device requires walking aids (crutches or a walker) to ensure stability and safety of the user. The FDA has recently approved a version of the ReWalk for use in the United States as a Class II (product class: powered exoskeleton) prescription device with special controls under 21 CFR Part 801.109 regulations. In December 2015, the US Dept. of Veterans Affairs issued a national coverage policy for the evaluation, training, and procurement of ReWalk Personal exoskeleton systems for eligible veterans with SCI4 .
3.7. WalkTrainer (SWORTEC, Switzerland, http://swortec.ch/index.php/products/walktrainer)
The WalkTrainer is equipped with bilateral and pelvic orthoses, active bodyweight support, closed-loop muscle stimulator and a mobile frame. The leg orthoses are comprised of a lightweight exoskeleton that is customized for each patient and is attached posteriorly by a powered mechanical leg via bar linkages (Stauffer et al 2009). The powered leg houses motors and mechanisms for actuating the hip, knee and ankle joints in parallel with the sagittal plane. The powered leg carries the entire actuator mechanism, cables, battery pack, etc making the patient's exoskeleton less bulky and thus enables the patient to freely move their arms during walking. The patient's feet are attached to the powered leg using foot plates that are embedded in the soles of specially modified shoes. The pelvic orthoses has six degrees of freedom which are actuated in co-ordination with the leg orthoses using foot switches to detect heel strike and toe off. Force sensors and potentiometers mounted on each axis of the exoskeleton help monitor the user's interaction with the orthoses and are used for implementing a selective compliant control algorithm. Additionally, a 20-channel real-time controlled muscle stimulator is used to augment the motion generated by the user and further, minimize the interaction forces between the user and the exoskeleton. The active body weight support ensures safety of patient during walking by precisely controlling the unloading force applied to the patient.
3.8. Wearable power-assist locomotor exoskeleton (WPAL; Fujita Health University, Japan)
WPAL has six degrees of freedom for bilateral flexion-extension at the hip, knee, and ankle joints. The level of the robotic hip joint is under the perineum, and it has an anterior-posterior curving slide mechanism that moves the virtual rotation center of the robotic hip joint closer to the center of the physical joint (Tanabe et al 2013b). Orthotic and robotic components are modular to allow orthotic components to be personalized whereas robotic components can be standardized for mass production. WPAL has one standing/sitting mode and three gait modes. Users can switch from simple gait mode to another optional mode (curve mode and slow mode) while walking by pulling a trigger or pressing a button. The curve mode allows the user to turn smoothly. In the slow mode, the step lengths of both feet are shortened. This mode is used for uneven surfaces. For patient safety, WPAL is used with a custom walker that provides stability during standing, walking and sitting. The walker also houses batteries, motor drivers and computer for controlling the exoskeleton via a wired interface (Tanabe et al 2013a).
A summary of the mechanical and controller characteristics of these powered exoskeletons is provided in table 1. Though marked differences exists across the different exoskeletons reviewed above, some common features for the exoskeletons can be drawn from these designs: currently, the mainstream exoskeleton design provides 1–6 degrees of freedom in the sagittal plane to drive the user's hip, knee, and sometimes ankle joints to follow desired gait trajectories during locomotion. Six of the systems integrate passive or active actuators at the ankle joint to facilitate dorsiflexion and plantar flexion. Generally, the user will partially depend on crutches, or a walker to support their weight and maintain balance, and joint angles and foot contact forces are often recorded to monitor basic gait performance. Based on the available information, all devices weigh less than 25 kg, and are operated with an auxiliary weight-supporting device such as forearm crutches or walker or body-weight support. The systems can be adjusted to the user's anthropometry to accommodate heights between 145–191 cm and a mass less than 136 kg.
4. Analysis of powered exoskeletons studies for SCI population
In this section, the 22 powered exoskeletons studies selected above are analyzed based on the protocol design, subject demographics, study duration, and primary/secondary outcome measures for assessing exoskeleton's performance in SCI patients. These factors are summarized in table 2 for each of the selected studies and discussed in detail below. The shaded rows in table 2 distinguish clinical studies (based on NIH's revised definition in section 2) from feasibility or preliminary evaluation studies that were included here for completeness.
Table 2. Selected studies of powered exoskeletons for SCI with outcomes measures.
| Experimental protocol | Subjects | Outcome variables | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | Reference | Device | Number of sessions | Duration in hours | Frequency per week | Duration in weeks | Number | Age | Injury level | Time since injury in years | 10 mWT | 6 minWT | TUG |
| 1 | (Bishop et al 2012) | Bionic Leg | 7 | 1 | — | 2 | 1 | 22 | C5/C6 | 4 | ▼ | △ | ▼ |
| 2 | (Kozlowski et al 2015) | Ekso | 8–24 | 2 | 1–2 | — | 7 | 21–49 | T8,C8,C4,L1,T9,T9,T10 | 0.4–7.4 | — | — | — |
| 3 | (Kolakowsky-Hayner et al 2013) | Ekso | 6 | 0.33–1.0 | 1 | 6 | 7 | 19–40 | T11,T10,T11,T7,T12,T4,T8 | 0.2–1.5 | — | — | — |
| 4 | (Kressler et al 2014) | Ekso | 18 | 1 | 3 | 6 | 3 | 26–38 | T1/T2,T7,T9/T10 | >1 | — | — | — |
| 5 | (Cruciger et al 2014) | HAL | 24–36 | 0.5–0.75 | 2–3 | 12 | 1 | 34 | T10 | — | — | — | — |
| 6 | (Kubota et al 2013) | HAL | 16 | 1.5 | 2 | 8 | 8 | 31–69 | — | 1.1–6.3 | △ | — | ▼ |
| 7 | (Tsukahara et al 2015) | HAL | 6 | — | — | 3 months | 1 | 39 | T7/T8 | — | △ | — | — |
| 8 | (Aach et al 2014) | HAL | 51.75 ± 5.6 | — | 5 | 3 months | 8 | 36–63 | T8,L1,T12,L1,L1,L2,T11,T12 | 1–19 | △ | △ | △ |
| 9 | (Farris et al 2014) | Indego | 1 | — | — | — | 1 | 42 | T10 | 10 | △ | △ | △ |
| 10 | (Evans et al 2015) | Indego | 2 | — | — | — | 5 | 28–51 | T7,T8,T10,T12,T6 | 1–20 | — | X | — |
| 11 | (Hartigan et al 2015) | Indego | 5 | 1.5 | — | — | 16 | 18–51 | C5,C6,C6,T5,T7,T5,T6,T7,T12, T10,T10,T11,T9,T12,L1,T12 | — | X | X | — |
| 12 | (del-Ama et al 2014) | Kinesis | 3 | — | — | 2 | 3 | 35–43 | L1,L2,L5 | — | △ | △ | — |
| 13 | (del-Ama et al 2015) | Kinesis | 3 | — | — | — | 3 | 35–43 | L1,L2,L5 | — | X | X | — |
| 14 | (Esquenazi et al 2012) | ReWalk | 13–26 | 1–1.5 | 3 | 8 | 12 | 18–55 | T8,T3,T8,T11,T10,T10,T4,T6,T10,T12,T7,T4 | 1–24.3 | X | X | — |
| 15 | (Fineberg et al 2013) | ReWalk | 11–45 | 1–2.0 | 3 | 5–6 months | 6 | 24–62 | T4,T1,T4,T8,T11,T5 | 1.5–14 | — | — | — |
| 16 | (Asselin et al 2015) [NCT01454570] | ReWalk | 12–54 | 1–1.5 | — | — | 8 | 24–61 | T4,T8,T11,T5,T1,T9,T7,T2 | 1.5–14 | — | X | — |
| 17 | (Zeilig et al 2012) | ReWalk | 7–24 | 0.83 | — | 3 months | 6 | 21–48 | T5,T7,T7,T9,T10,T12 | 3–7 | X | X | X |
| 18 | (Benson et al 2015) [NCT01943669] | ReWalk | 20 | 2 | 2 | 10 | 5 | 23–41 | L1,T12,C7,C8/T2,T9 | 1.4–7.25 | △ | △ | △ |
| 19 | (Yang et al 2015) [NCT02118194] | ReWalk | 12–120 | 1–2.0 | 1 | 12 | 12 | 24–64 | T4,T10,T4,C8/T8,T11,T5,T1,T9,T7,T2,T2,C8 | 1–16 | X | X | — |
| 20 | (Stauffer et al 2009) | Walk-Trainer | 12 | 1 | 1 | 12 | 6 | — | — | — | — | — | — |
| 21 | (Tanabe et al 2013a) | WPAL | 2–11 | 1 | — | — | 7 | 32–61 | T12,T12,T11,T9,T6,T6,T6 | 6–20 | X | — | — |
| 22 | (Tanabe et al 2013b) | WPAL | 6–39 | 1 | 2–3 times/month | 3–13 months | 4 | 30–59 | T12,T11,T6,T12 | 4–20 | — | X | — |
Note: Outcome variable symbols: △: positive change; ▼: negative change; X: no comparison; —: data not available;ClinicalTrials.gov registered study identifier shown in parenthesis [ ]; shaded rows indicate clinical studies; Unshaded rows indicate feasibility or preliminary evaluation studies.
4.1. Protocol designs varied across studies
Inspection of the session protocol across studies revealed large differences in the number of sessions and overall duration of experiments. The maximum number of sessions across all studies was 120, yet a fraction of these were used for training the subject in operating the exoskeleton (Yang et al 2015). A single session study among the twenty-two studies is also present (Farris et al 2014). Typically, the number of sessions per week was two to three, with only one study conducting experiments five days per week (Aach et al 2014). The duration of individual sessions ranged between one to two hours, with no studies reported exceeding two hours per session.
4.2. Distribution of SCI subjects by level of injury differed across studies
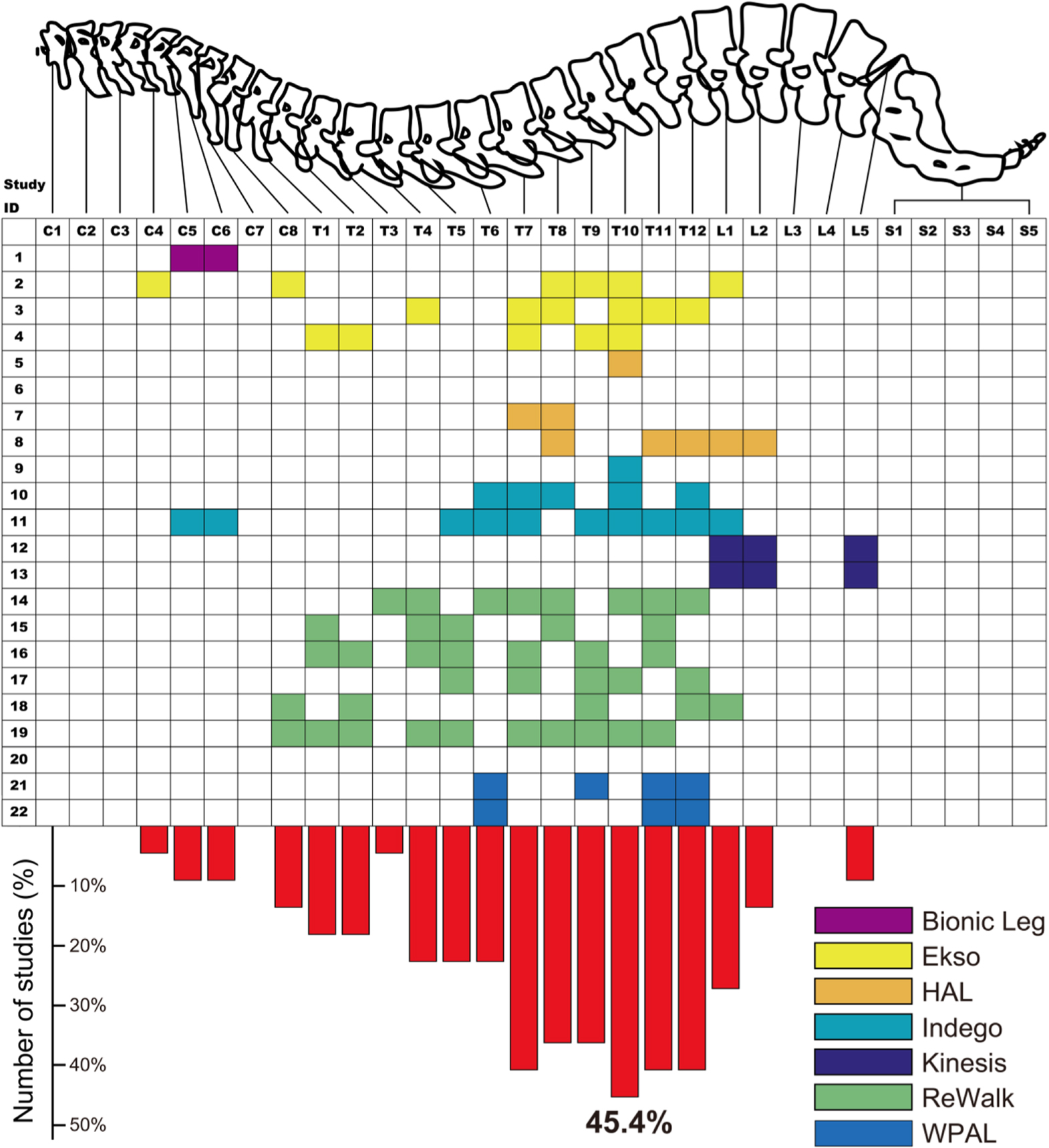
Table 2 also shows the distribution of subject demographics, including number of subjects, their ages, injury level and time since injury. One of the biggest sources of discrepancy among these studies is in the number of participants enrolled. The average number of subjects was six with a standard deviation of four subjects, ranging between one and sixteen study participants. Among the 22 studies, four reported findings based on single subject data, with one of those being a single session experiment. Interestingly, table 2 shows a wide range of SCI injury levels included in these studies. This is also evident in figure 1, which shows the distribution of level of injury across all the studies. Figure 1 reveals that a majority of studies included patients with thoracic level injuries, amongst which patients with T10 injury were present in 45.4% of studies. Five of the studies reported include patients with cervical level injuries, whereas none of studies recruited patients with sacral level injury. The time since injury reveals, that most of the studies recruited chronic (≥6 months) SCI subjects with the exception of (Kolakowsky-Hayner et al 2013, Kozlowski et al 2015) which also recruited acute SCI subjects.

Figure 1. Distribution of SCI injury level in participants of studies with powered exoskeletons.
Download figure:
Standard image High-resolution image4.3. Outcome measures focused on assessing mobility
Seven primary measures associated with functional ambulation in SCI patients were identified by a recent survey (Lam et al 2011): 10 meter walk test (10 mWT), 6 minute walk test (6 mWT), timed up and go (TUG), spinal-cord injury functional ambulation inventory (SCI-FAI), functional independence measure, Spinal cord independence measure, and walking index for spinal cord injury (WISCI-II). Of these, the first three are timed measures, and the latter three are categorical assessments of ambulation, with the SCI-FAI having components of both. The experimental design of the studies presented in this review host a variety of outcome metrics including these seven measures, as well as other metrics aimed to assess physiological and psychological changes, and usability. Since the 10 mWT, 6 mWT, and TUG tests were administered by a majority of the studies (as seen in figure 2), we additionally report these tests in table 2 and compare their outcomes. Further, we split the primary and secondary outcomes of all studies into five categories: quantitative functional ambulation assessments covers timing-based measures related to functional walking; balance and level of assistance/independence considers functional ambulatory measures incorporating the categorical assessments and balance tests; physiological improvements include measures studying effects related to muscle, spasticity and bowel/bladder function; energy expenditure during use covers metrics looking at the energy required when using the exoskeleton; and usability and comfort address the device ergonomics.

{kind=link}
Figure 2. Categorical distribution of outcome measures used in studies.
Download figure:
Standard image High-resolution image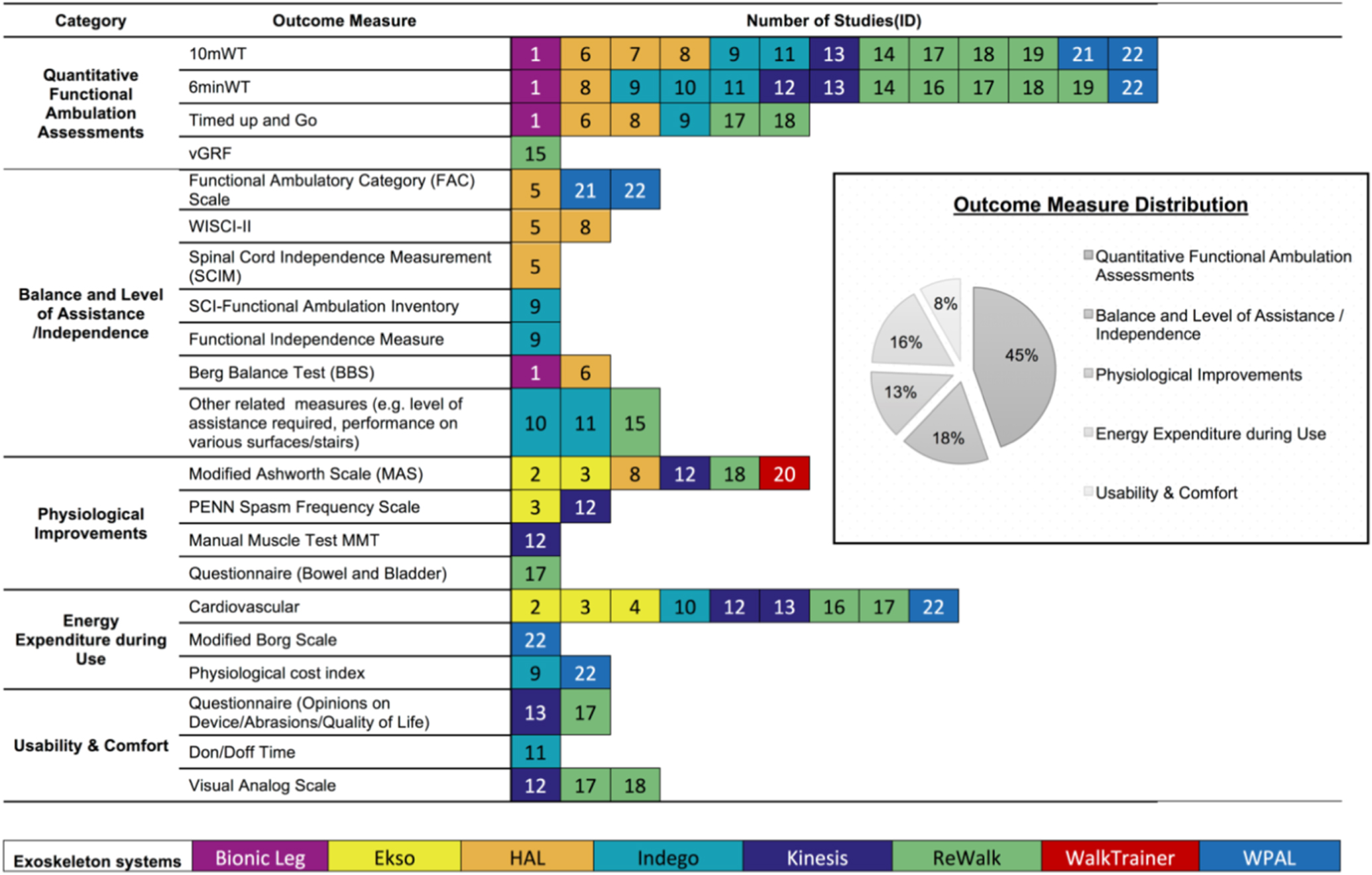{kind=link}
Figure 2 shows the categorical breakdown of all the outcome measures used in the selected studies, as well as the distribution of each category. It can be noted that 63% of the outcome measures selected are gait and ambulation related, with researchers emphasizing quantitative measures (45%) over outcome measures evaluating balance, level of assistance and independence (18%). This is followed by outcome measures measuring energy expenditure (16%), physiological improvements (13%), and usability and comfort (8%). Overall, studies with the largest number of outcome measures were based on ReWalk (20 measures across six studies), followed by Indego (13 measures across three studies), HAL (12 across four studies), and Kinesis (10 across two studies).
4.4. Overall comparison between studies
When comparing experimental designs, there is a general consistency across all studies in the number of sessions per week (1–3/week) during which the exoskeleton-based intervention was provided. The treatment frequency is also consistent with traditional locomotor training (e.g. robot-assisted gait training) frequency of 2–5 sessions per week (Wirz et al 2005, Schwartz et al 2011). Interestingly, (Aach et al 2014) implemented their exoskeleton therapy for five sessions per week and observed a positive change in the three most commonly used outcome measures (10 mWT, 6 minWT, TUG). Five out of seven studies that compared metrics pre- and post-intervention, report improvement from baseline, whereas two studies reported negative change (see table 2). Unfortunately, due to wide variation in metrics, number of subjects, level of injury and training protocols, the information available is not sufficient to make specific comparisons between these studies. For example, there is no consensus on the duration for which the exoskeleton therapy must be applied. Training duration varied from single trial evaluations (Farris et al 2014) to longitudinal studies with many subjects training over many sessions for more than two months (e.g. Esquenazi et al 2012, Fineberg et al 2013, Yang et al 2015). Future studies should be designed to be consistent in the duration of intervention (total number of sessions, sessions per week, and session duration), in order to allow more meaningful comparisons. Moreover, based on published results that reported positive changes in outcome variables (see entries in table 2), a recommended dosage of 2 h per session, for at least 20 sessions is recommended as it has been noted that increases in gait speed using powered exoskeletons are correlated with training time (Louie et al 2015).
5. Discussion
5.1. Level of injury of the SCI population should be better represented in future studies
According to the National Spinal Cord Injury Statistical Center, more than a half of SCI patients have cervical injuries, with C5 as the largest category, followed by thoracic level injury (T1-T12) (NSCISC 2015). However, as pointed out in this review, a majority of the studies focus on thoracic level SCI and future studies focusing on wider levels of injury including C1-C8, L2-L5, and S1-S5 are required. Yet, little is known about how the level of injury affects the usage of exoskeletons and it is likely that for safety reasons specialized designs (e.g., devices with alternative human–device interfaces, automatic gait intent detection mechanisms, upper body support, self-balancing designs, etc) will be needed for C-level patients with tetraplegia with poor upper-body control. Of note is that pediatric SCI patients were not included in this review as there were no studies that included SCI patients younger than 16 years old. The pediatric SCI population may have a greater potential for neurological recovery compared to adults and thus should be investigated as a potential group for training with these devices (Parent et al 2011). Thus, pediatric-centered designs of powered exoskeletons for over-ground walking should be considered in the near future.
5.2. Outcome measures should be comprehensive and consistent across studies of powered exoskeletons
Among the outcome measures evaluated in the selected studies, there was a general inconsistency in the metrics used. While some studies relied on standardized tests and timed measures to assess functional, physiological, or psychological improvements in their subjects, others relied on custom metrics and questionnaires or subjective observation-based assessments. This posed a significant impediment in objectively comparing devices and tracking their clinical efficacy and benefit to patients. The categorical classification of metrics (section 4.3) revealed that none of the studies had outcome measures spanning every category. Only two studies involving Kinesis (ID 12) and ReWalk (ID 17) had outcome measures that spanned four categories. It appears that the choice of outcome metrics used may be motivated by the preference of the researchers that conduct these studies. Farris et al (2014) mentioned this in their discussion, describing the lack of standardized metrics used by researchers in characterizing mobility and level of exertion in the use of assistive devices.
The review of the literature shows that there is an emphasis on ambulatory-related primary outcome measures, where both quantitative and qualitative measures focusing on gait and balance account for 63% of all measures in these studies. Indeed, the 10 mWT, 6 minWT, and TUG are known to be reliable, validated, and responsive (Lam et al 2011), and thus they should be considered in future studies that assess potential benefits of balance and walking ability using powered exoskeletons. In addition, a recent study suggests an adequate gait speed for community ambulation (e.g., to allow safe street crossings) to be 0.49 m s−1 and this should be taken into account as one of the measures for assessing mobility benefits in real-world scenarios (Andrews et al 2010). Improvements in bowel/bladder function, stability and strength were only alluded to in a few of these studies (Strausser and Kazerooni 2011, Zeilig et al 2012). A previous review of the outcomes of SCI research found similar pitfalls widely present across all areas of SCI research (Hammell 2010). The author in (Hammell 2010) observed that the SCI population felt that researchers may be overlooking many of the desired outcomes of the populations and replacing them with far-reaching goals, or worse, secondary or tertiary goals beyond their direct vision of improvement. Furthermore, the SCI population reported feeling that they were only part of a study that evaluated differences in outcome metrics and not in improvements in the QOL of the individual. Thus, it is discouraging to see that the target population, which the researchers are attempting to help, does not feel that they are being adequately represented in these studies. This is also a limitation of many of the studies presented in this review, which do not specifically address the improvements in QOL, but rather focus on changes within particular metrics related mostly to walking mobility. Thus, for a simple paradigm shift in future exoskeleton research for the SCI population, studies should broaden their scope, including metrics across multiple physiological systems as well as improvements in areas related to QOL and usability.
5.3. Perception of benefits of using exoskeletons by individuals with SCI
Although SCI patients generally consider it very important to walk again, it is unclear if the mobility benefits of powered exoskeletons (i.e., ability to stand up and walk) align well with the desired outcomes or expectations of the diverse SCI population (Benson et al 2015). In one study, 437 SCI survivors were asked to rate their difficulty in dealing with 10 consequences of SCI, on a scale ranging from 0 (not hard at all) to 10 (extremely hard). The highest rated five consequences were decreased ability to walk or move, decreased control of bowel, decreased control of bladder, decreased sexual function, and pain (means ranged from 8.2 to 6.2); moreover, high ratings of feeling sad were associated with high ratings of most other consequences (Widerstrom-Noga et al 1999). A poll (N = 681; 51% quadriplegic and 49% paraplegic; 25% female, 65% male) by Anderson in 2004 assessed the priorities in physical recovery after SCI directly from the patient population (Anderson 2004). The study concluded that sexual function, bladder and bowel function, walking movements, and trunk stability are priorities in the recovery process of SCI patients, but that the ranking of these priorities depended on whether the patient had paraplegia or tetraplegia. In particular, walking movements were prioritized by 15.9% of individuals with paraplegia compared to 7.8% of individuals with tetraplegia. Therefore, in addition to mobility, future studies should include metrics that evaluate the devices in a manner that directly complies with the desired outcomes of the SCI population. For example, none of the studies measured changes in sexual function, which is one of the most desired improvements of the SCI population (Anderson 2004).
Individuals with SCI often face challenges with social interactions, which may be overcome by use of an over-ground exoskeleton that allows legged locomotion, facilitates social interaction at eye level, and basic sitting and standing. In a survey of wheelchair users and healthcare professionals (Anderson 2004), 75% of the participants reported increased social interaction as a rationale for using an exoskeleton. The ability to carry out normal social interactions may provide enormous psychological benefit to individuals who may otherwise be limited in social environments. This possibility is however rarely assessed in current studies of exoskeletons.
Although use of exoskeletons is focused on ambulation and lower limb motor improvement, there may be secondary benefits across multiple physiological systems, such as improved bowel/bladder function, decreased chronic pain, reduced spasticity, and increased bone marrow density (BMD). Some of the clinical trials in this review (Zeilig et al 2012) found that users of the device reported an improvement in bladder and bowel function after training with the ReWalk, although none of these studies provide conclusive evidence. Additionally, it is believed that using these devices can lead to a reduction in chronic pain and spasticity (Esquenazi et al 2012, Zeilig et al 2012), but this needs to be confirmed. Decreased BMD is a common symptom in SCI patients (Dolbow et al 2011) and degradation becomes rapidly evident within the first year of sustaining the injury (Coupaud et al 2015). Dolbow and colleagues report that passive loading of the lower limbs alone (such as during standing) does not result in increased BMD and thus additional methods of stimulation may be required to induce bone growth (Dolbow et al 2011). Stressing the bone through muscle contractions, such as natural muscle contractions induced through walking or artificial contractions by FES, shows potential for increasing BMD in non-weight bearing individuals (Dolbow et al 2011, Bryce et al 2015). The use of an over-ground powered exoskeleton does not specifically activate muscle contractions in users (although residual EMG can be detected in some SCI patients during exoskeleton use); however, it is possible that active stimulation through ambulation in an exoskeleton can result in increased BMD, or at least attenuate any further loss after extended use. Thus, hybrid exoskeletons (e.g. Kinesis and WalkTrainer) that combine mobility with FES may provide these benefits. Moreover, future powered exoskeletons could be explicitly designed to target benefits across multiple physiological systems, which may lead to wide spread adoption of this technology by patients, physicians and insurance providers.
5.4. Medical device regulation of powered exoskeletons
Careful consideration of outcome measures is not only important to evaluate the impact of exoskeleton intervention on patients, but also required for obtaining marketing clearance from appropriate regulatory authorities. In United States, powered exoskeletons are classified as Class II devices and require premarket notification 510(k) clearance from the FDA before they can be marketed (Food and Drug Administration, HHS 2015). Currently, ReWalk is the only over-ground walking exoskeleton to receive FDA approval (http://accessdata.fda.gov/cdrh_docs/reviews/den130034.pdf) for home use for people with paraplegia due to SCI at levels T7-L5 when accompanied by a specially trained caregiver. In addition, it can also be used in rehabilitation institutions for ambulation of SCI patients with T4-T6 injury. However, the device is not approved for sporting activities or climbing stairs. Additionally, patients and their caregivers are required to undergo extensive training developed by the manufacturer to learn and demonstrate proper use of the device. The new FDA regulation implies that it will regulate all powered exoskeletons as Class II (moderate to high risk) devices, meaning that they are subject to general and special controls prior to FDA approval, rather than Class I (low to moderate risk) devices that are subject only to general controls.
The approval of ReWalk by the FDA can be considered pivotal in many ways. First, it can increase the acceptance of and confidence in powered exoskeletons among the health care industry as well as users. Second, it will simplify to a certain extent the path to commercializing exoskeletons, since any new device, which can demonstrate to be 'substantially equivalent' to ReWalk, can be readily approved by the FDA. According to a recent press release (http://ir.eksobionics.com/press-releases/detail/444/ekso-bionics-to-submit-510k-notification-in-december), Ekso Bionics submitted a 510(k) application to the FDA in December 2014 and the company has been allowed to continue to market the device while the 510(k) submission is under review. Quite recently (8 March 2016), the FDA also released 510(k) premarket notification for the Indego exoskeleton, thus allowing Parker Hannifin Corporation to market the device, subject to the general controls provisions of the Federal Food, Drug, and Cosmetic Act. Nonetheless, all exoskeletons reviewed here (except ReWalk) have yet to demonstrate their safety and efficacy and satisfy special controls as required by the FDA. As clinical trials are completed and longer interventions are performed, probable benefits and probable risks will be confirmed or disconfirmed.
5.5. Outlook
It is becoming clearer that worldwide markets are likely to achieve significant growth as powered exoskeletons are used inside rehabilitation centers and are deployed in homes and outdoors. According to a recent market study by WinterGreen Research, the rehabilitation robot market size is expected to reach $1.1 billion by 2021, with the specialized exoskeleton market to be considered as separate and additive to this market (WinterGreen 2015). Although an increasing number of companies are conducting clinical trials to obtain regulatory approval in the US, Europe and Asia, there is no clear dominance of the exoskeleton market. The most advanced systems that are currently being marketed are still emerging as commercial devices, and specialized market applications are still being evaluated.
It is generally agreed that locomotor training using robot-assisted therapies depends on patient engagement (Venkatakrishnan et al 2014), reward (Goodman et al 2014) and the desire of the patient to conquer the disability. Thus, wearable robots that engage the patient with gait intent detection can help motivate the patient, provide short-term reward via immediate feedback of movement, and empower the patient with direct control of his/her own health and QOL (Krebs et al 2003, Blank et al 2014). Towards this extent, gait intention detection systems for exoskeleton control, such as by monitoring shifts in the center of mass (e.g. tilting the trunk) (Zeilig et al 2012), may improve the efficacy of rehabilitation by encouraging the user to actively participate rather than relying solely on the assistance provided by the exoskeleton. Other gait intent detection systems based on eye gaze (Duvinage et al 2011) and hand movements (Hasegawa et al 2009), have also been developed. More recently, development of peripheral or brain neural interfaces for automated gait intent detection and closed-loop control involving both of these systems (Suzuki et al 2007, Fitzsimmons et al 2009, Wieser et al 2010, Presacco et al 2011, 2012, Wagner et al 2012, Kilicarslan et al 2013, Bulea et al 2014, He et al 2014, Kwak et al 2015), are also being explored. These emergent human–robot interfaces may be critical in augmenting the range of users of such devices, including subjects with tetraplegia.
In addition, it is critical that new exoskeleton designs scrutinize the metabolic and biomechanical cost of human walking assisted by powered exoskeletons. Extended use of these systems can lead to overuse injuries of the upper-body, and physical and mental fatigue. These aspects were however, rarely assessed in the studies reviewed here. Two recent studies have shown in able body subjects that exoskeleton designs can significantly reduce the metabolic cost of walking (∼8%) relative to not wearing an exoskeleton (Mooney et al 2014); even in the case of passive exoskeletons (Collins et al 2015). Secondary outcome measures should also be considered in future exoskeleton design. Although different assessments were conducted to evaluate the impact of exoskeleton intervention on patients' pain, fatigue, and comfort levels before and after the robot intervention, the systems themselves reviewed here did not have sensors integrated into the system that could directly monitor these dynamics in real time. Recently, (Tamez-Duque et al 2015) presented a system to monitor the pressure exerted on the user by the leg straps of the exoskeleton. This is important as recent studies have reported grade I/II skin aberrations in five out of ten enrolled subjects (Benson et al 2015), and bruising and grade-1 skin redness in two patients during exoskeleton use (Hartigan et al 2015). Additionally, usability metrics such as the training period, i.e. time required by patients to learn to use a powered exoskeleton, can help in the design of future interventions (Bryce et al 2015). For example, in (Kozlowski et al 2015), the authors quantified the training period in terms of number of sessions required to use the exoskeleton to stand up, walk for at least 30 min, and sit down with little or no assistance. The authors concluded that up to eight (median, 95% CI = 5.4–10.6) sessions were required by six participants with cervical and thoracic level injuries to learn to use the exoskeleton with minimal assistance, which may be correlated with age and time since injury (Kozlowski et al 2015).
Safety considerations are yet another important aspect in the design of powered exoskeletons. Risks of falling, tripping and slipping not only endanger the safety of patients using the exoskeleton but also have social, emotional, and psychological consequences (Tucker et al 2015). These incidents can arise due to internal factors (e.g. controller failure) or external factors (e.g. uneven terrain, moving objects or persons). Current approaches to prevent such risks include mechanical stops/limit switches (e.g. Kinesis) or use of walkers and crutches (e.g. Bionic Leg, Ekso, ReWalk, HAL, Indego, WPAL). WalkTrainer uses an active body-weight support. In the reviewed studies, except for a single report of near-serious adverse event (Benson et al 2015), none of the studies reported any adverse events as a result of falling or slipping. This suggests that the current approaches to prevent falls during training with current devices may be effective and should be continued in future studies. Furthermore, five studies (IDs: 1, 2, 11, 18, 19) reported in this review were conducted with subjects with cervical lesions, out of which four where clinical studies (IDs: 1, 2, 18, 19). This suggests that it is feasible to include cervical level subjects and despite their injury they may retain the ability to use crutches and other body support systems. Moreover, subjects completely lacking this ability could benefit from self-balancing exoskeletons such as Rehab REX (from Rex Bionics; see http://rexbionics.com/) and advanced human–machine interface systems for detecting gait intention as discussed above.
Overall, a user-centered design of powered exoskeletons is needed, which involves the development of innovative science and technologies that minimize the mismatch between the sensorimotor capabilities of the user and the exoskeleton, leading to their intuitive integration and confluent interaction. To gain adoption by end users, exoskeletons should be effective, reliable, safe and engaging and support the user in performing intended actions with minimal effort and errors with adequate interaction time (Contreras-Vidal et al 2015). Although significant advances in the design of powered exoskeletons have been achieved in the last decade, current systems have not yet reached the level of performance required to function in complex dynamic environments, usually require extensive training and/or a trained staff to set-up or operate, put insufficient emphasis on understanding long-term system-level plasticity, and do not readily adapt to changing effects of the patient's neurological status, biomechanical condition, attention, and fatigue. Moreover, the long-term reliability of powered exoskeleton is currently unknown, and the lack of standard metrics to quantify their effectiveness and reliability impede fast translation to the end-user.
6. Conclusions
This systematic review focused on published literature of powered exoskeletons for bipedal locomotion in individuals with spinal cord injury. A total of twenty two studies with eight powered exoskeleton systems met the inclusion criteria for review. As depicted in table 1, many of these systems are rather similar in design, focusing on lightweight frames with actively powered hip and/or knee joints. Seven of the eight of the exoskeletons reviewed in this study, are bilateral systems with active actuators at the hip and knee joints in the sagittal plane (except for Kinesis, which does not actuate the hip), whereas Bionic Leg is a unilateral RKO. The current technology for over-ground exoskeletons is relatively new and specific benefits of long-term use of exoskeleton in gait training still remains to be elusive. Several of the studies reviewed here are still in feasibility and development stages. For a more holistic assessment on how exoskeletons can be applied alone or together with conventional rehabilitation therapies for effective recovery, outcome measures for future studies should expand their assessment metrics to account for more physiological and usability measures as well as maintain consistency by using standardized metrics for assessing safety, benefits, and usability. Studies should also develop criteria for optimal selection and training of patients most likely to benefit from a particular device and make use of the array of sensors embedded in exoskeletons to develop real-time monitoring and diagnostic capabilities that can inform the physician while allowing adjustment of the device according to the needs of the user.
Acknowledgments
This work was supported in part by NINDS Awards R01NS075889, Mission Connect—TIRR Foundation.
Footnotes
- 3
During online search on ClinicalTrial.gov we did find a clinical trial (NCT02417532) registered for REX exoskeleton (Rex Bionics, New Zealand). As compared to other exoskeleton reviewed in this study, REX's unique self-balancing feature is noteworthy. However, since this study does not have any published results at this time, we exclude it from this systematic review.
- 4
Memorandum from Department of Veterans Affairs (VA) can be found online at http://sci.va.gov/docs/VHAReWalkStatement_cleared.pdf. The VA has recently listed a national, multi-center study utilizing the ReWalk Personal 6.0 exoskeleton system (www.clinicaltrials.gov Identifier: NCT02658656).